The impact of THC and CBD on schizophrenia
Background: People with schizophrenia are more likely to develop cannabis use disorder (CUD) and experience worse outcomes with its use. However, since cannabis is legalized for both medical and recreational use, there is interest in its therapeutic potential.
Objectives: To conduct a systematic review summarizing the design and results of controlled studies using defined doses of THC and CBD in schizophrenia.
Method: A keyword search in eight online literature databases identified 11 eligible reports.
Results: A placebo-controlled study (13 stable patients without CUD) found that intravenous THC increased psychosis and worsened learning/memory. Two reports from a functional magnetic resonance imaging (fMRI) study of smoked or oral THC in 12 abstinent patients with schizophrenia and CUD found no change in symptoms and cognition, and an improvement in impaired resting-state brain function in areas implicated in reward function and pattern mode network. A 4-week study in acute psychotic patients without CUD (mean age 30 years) found that 800 mg of CBD is equally effective as amisuprida in improving psychosis and cognition. Two 6-week studies of antipsychotic augmentation with CBD in stable outpatients reported mixed results: CBD 600 mg was no more effective than placebo; CBD 1,000 mg reduced symptoms in a sample that did not exclude the use of cannabis and CUD.
Discussion: There is substantial heterogeneity among the studies regarding dosage, method of drug administration, duration of treatment, patient age, whether patients using cannabis/CUD were included or excluded, and whether patients were using antipsychotic medication.
Conclusion: There is insufficient evidence for an effect of THC or CBD on symptoms, cognition, and neuroimaging measures of brain function in schizophrenia. Currently, research does not support the recommendation of medicinal cannabis (THC or CBD) for the treatment of patients with schizophrenia. Further research should examine THC and CBD in schizophrenia with and without comorbid CUD and consider the role of CBD in mitigating the exacerbation of THC symptoms.
Introduction
Schizophrenia is a chronic neurodevelopmental disorder experienced by 0.5 to 1.0% of the population worldwide. 1 , 2 ). This condition typically begins in late adolescence or early adulthood and includes positive symptoms, such as hallucinations, and negative symptoms, such as avolition. Cognitive impairments, such as attention and working memory problems, are central features of schizophrenia, and an impaired ability to anticipate rewards has also been documented. 3 ). Anxiety Significant change is common, although it is not a central symptom of schizophrenia. ( 4.5 ). Substance use disorders are more common in people with schizophrenia than in the general population, and marijuana is the most common illicit drug used by people with this condition. 6 – 9 ). Up to 43% of people with schizophrenia develop a cannabis use disorder (CUD). 10 – 13 ) compared to 6.3% in the general population ( 14 ).
Interestingly, epidemiological studies have shown that heavy cannabis use in early adolescence is associated with an increased risk for the development of new psychotic symptoms and schizophrenia spectrum disorders ( 15 – 19 ). A dose-response relationship was observed, with a higher incidence of schizophrenia found in heavy cannabis users compared to light users or non-users. 17 ). Furthermore, among people who have an established schizophrenia spectrum disorder, observational studies have shown that recreational cannabis use and cannabis use disorder are associated with worse symptoms and disease course ( 20 – 23 ). As we will outline further below, examining the effects of THC and CBD, alone and together, can help to better understand the mechanism of action of cannabis effects, the pathophysiology of schizophrenia, and whether there is any therapeutic role for these components of cannabis in people with schizophrenia with and without cannabis use disorders.
Cannabis is a genus of plants with various species containing over 100 types of cannabinoids. The strains are bred to promote varying levels of cannabinoids, especially (-)- trans -Δ 9 Tetrahydrocannabinol (THC) and cannabidiol (CBD), which have different effects. THC is responsible for the intoxicating “high” from cannabis and is likely a component of cannabis responsible for the development of CUD in about 10% of users [for review, see (24) ] . In contrast, CBD does not appear to cause intoxication, nor is it a high (high). 25 , 26 ).
Controlled laboratory studies in healthy participants have demonstrated that THC administration results in acute psychotic symptoms and dose-related transient cognitive impairments, including in working memory and executive control of attention, in up to 50% of healthy individuals ( 27 ), and for review, see ( 28 ). Some studies show a dose-related effect for psychosis [for example, ( 27 )]. Pretreatment with CBD has been shown to mitigate such symptoms and deficiencies induced by THC ( 29 – 32 ), but not the positive and reinforcing effects ( 26 ). Notably, the THC content in typical street cannabis increased from ~4% in 1995 to ~12% in 2014 ( 33 ), and the ratio of CBD to THC has decreased to almost zero in many strains, although strains with high CBD content are also available ( 34 ). THC and CBD are used to create a variety of high-potency products for sale, especially in places where medicinal and recreational cannabis is legal. Therefore, readily available recreational cannabis with high THC content has a strong potential to cause negative effects.
Although recreational cannabis use (supposedly high in THC and low in CBD) has been associated with worse outcomes in schizophrenia, several case reports have suggested that CBD itself may be beneficial in treating psychosis. 35 , 36 ). A more recent cross-sectional report indicated that the use of high-CBD cannabis was associated with significantly fewer psychotic symptoms in patients with schizophrenia ( 32 ). Research using animal models examining the antipsychotic properties of CBD has determined that CBD leads to behavioral responses similar to those to an atypical antipsychotic medication. 35 ), contributing to the interest in testing CBD for its ability to improve symptoms in patients with schizophrenia.
As Canada and parts of the US have legalized cannabis for recreational (16 states as of 2021) or medical (12 states as of 2021) purposes 37 Since then, cannabis production and sales have skyrocketed, and the public increasingly perceives cannabis as beneficial rather than harmful. Recent research has shown that nearly half of Americans said they believe cannabis can alleviate anxiety and depression. 38 ). Thus, in places where marijuana is legal for recreational or medical use, many people seek it out to treat mental health problems. For example, in a US report, more than a third of people who used medical cannabis reported using it to reduce anxiety ( 39 ), and several Canadian studies have reported that cannabis is widely used to treat anxiety, depression, and sleep ( 40 , 41 ), common symptoms in a variety of mental health conditions, including psychotic disorders ( 42 ).
Thus, as stakeholders become increasingly interested in the potential therapeutic effects of cannabis, they need reliable information about the effects of THC and CBD, particularly among vulnerable populations such as people with schizophrenia. Several previous reviews have addressed the effects of THC or CBD in people with schizophrenia ( 43 – 50 ). We seek to provide an up-to-date review, as well as a detailed and critical review of the literature, including studies of CBD and THC considered together, as well as a critical review of the research methods, research quality, and direction of the evidence for each study. 51 ), focusing on randomized controlled trials (RCTs), as they provide the highest level of evidence. This review, therefore, provides an overview of the evidence regarding the potential benefits and harms of THC and/or CBD in schizophrenia to date. We conducted a systematic review of published prospective and controlled studies testing the impact of THC and/or CBD on symptoms, cognition, and neuroimaging measures of brain function in people with schizophrenia spectrum disorders.
Methodology
Source of information and research
Bibliographic searches using PubMed/MEDLINE, PsycINFO, PsycARTICLES, CINAHL, EMBASE, Scopus, Cochrane, and Academic One File were conducted for English-language articles published between January 1, 1970, and June 15, 2021. Search terms included: “cannabidiol AND schizo * "; "cannabidiol and psycho * "; "CBD and schizo * "; "CBD and psycho" * "; "tetrahydrocannabinol and schizo * "; "tetrahydrocannabinol and psycho * "; "THC and schizo * "; "THC and psychopath" * .” In addition, we examined recent peer-reviewed scientific reviews of the literature on cannabinoids and psychosis, as well as reference sections of articles obtained from online literature searches, for any other relevant articles.
Inclusion and exclusion criteria
All studies reporting prospective RCTs testing specific doses of whole-plant cannabis, CBD, THC, or both compounds compared to placebo or a control condition with standardized assessments of psychosis symptoms, cognition, and/or neuroimaging in humans with schizophrenia spectrum disorders were considered. Any commercially available or synthetic formulation of THC or CBD was accepted, as well as any route of administration for any length of time. Age, gender, and race/ethnicity were not included in the selection criteria. We excluded cross-sectional studies, observational studies without a control condition, studies that examined cannabis that did not use a specific dose of THC and/or CBD, CBD used for psychiatric conditions other than schizophrenia, and articles not written in English. studies that do not report original research,
Study quality assessment
After the studies were selected, we performed a quality assessment of the study using a checklist for the "Grading, Recommendation, Development and Evaluation (GRADE)" approach. 51 GRADE is a transparent and widely used grading system for evaluating research quality and developing evidence summaries that provide a systematic approach to making clinical practice recommendations. 52 – 54 We use two categories: study quality/risk of bias and objectivity/indirectness of the evidence.
Results
Study selection
The initial survey yielded 6,003 reports. After removing duplicates, the studies were selected based on their titles, resulting in the inclusion of 722 citations. The abstracts were then screened, resulting in the exclusion of 512 citations. The remaining articles (235) were reviewed for eligibility by two authors (CNS and SA). Any disagreements were mediated by a third reviewer (MB). A total of 226 articles did not meet the inclusion criteria, resulting in 11 full-text articles that met the inclusion criteria. The selection steps are shown in Figure 1 .
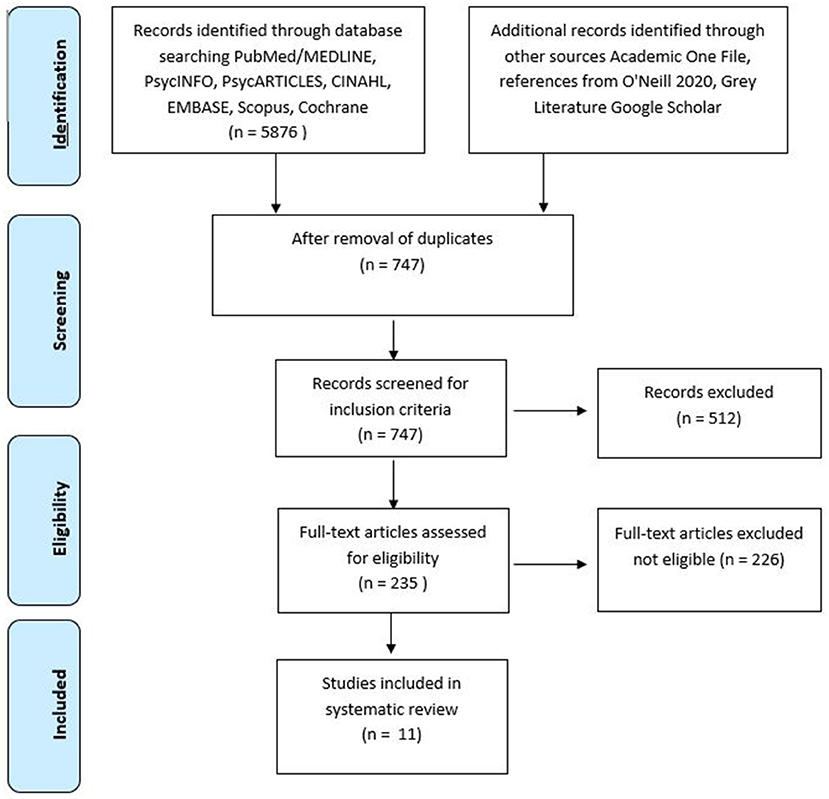
FIGURE 1 . Flowchart.
Study characteristics
Table 1 It provides the characteristics of nine prospective placebo-controlled studies of cannabis, CBD, and/or THC. These studies were published between 2005 and 2021 and employed a variety of methods, described in the table and below.
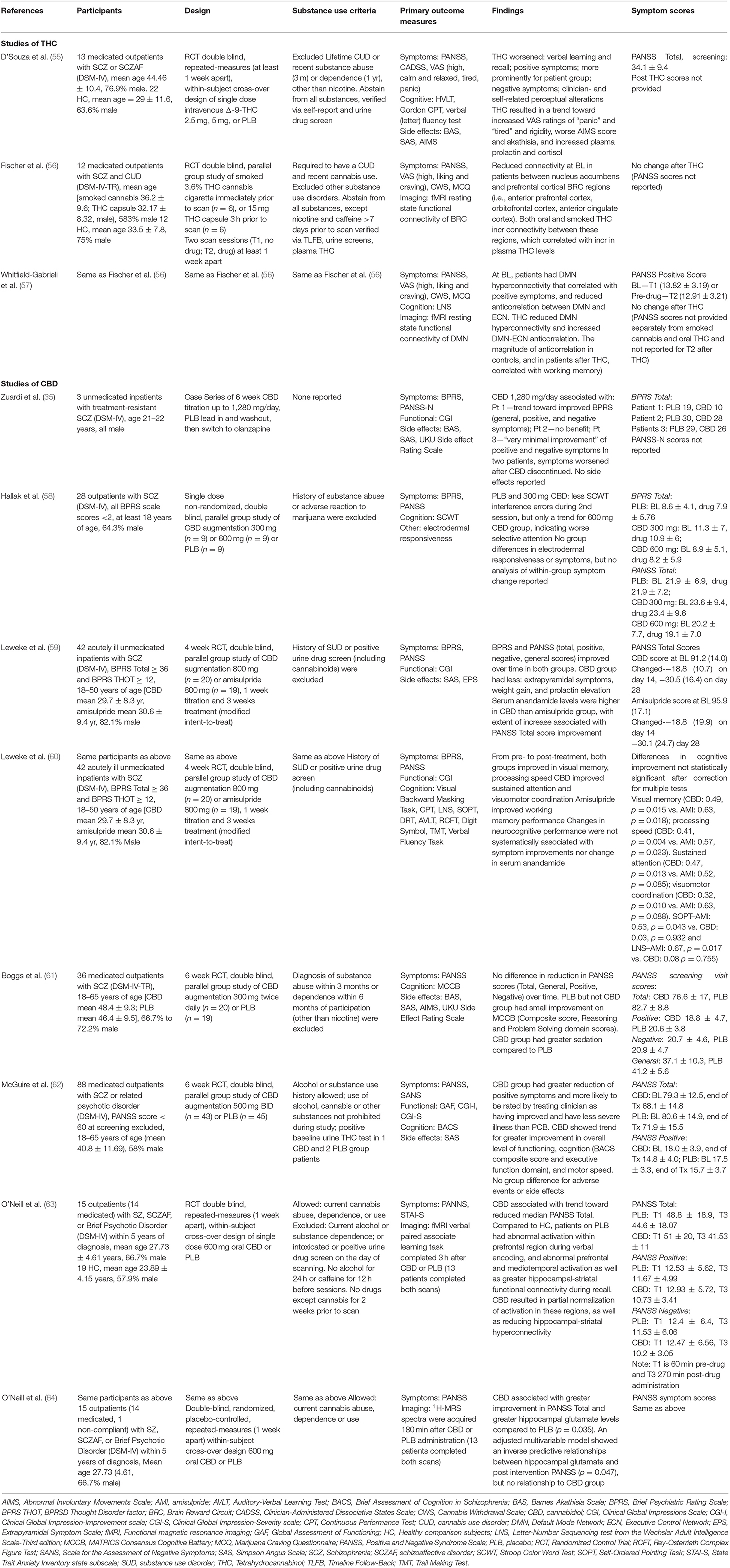
TABLE 1 . Methods and results of studies on CBD and THC in the treatment of schizophrenia.
Characteristics of CBD studies
Four RCTs (reported in six articles) met the inclusion/exclusion criteria. Three were longitudinal treatment studies lasting 4 to 6 weeks ( 59 , 61 , 62 ) and one was a single-dose laboratory study reported in two articles that used functional magnetic resonance imaging (fMRI) ( 63 ) and proton magnetic resonance spectroscopy (1H - MRS) ( 64 ). We also included a single, non-randomized, balanced study assessing cognition ( 58 ) and a series of placebo-controlled crossover treatment cases of three patients ( 35 ). Four of these RCTs evaluated CBD vs. placebo for antipsychotic potentiation ( 58 , 61 – 64 ), while another compared CBD to amisulpride in patients with acute illnesses who had not been on antipsychotics for at least 3 days, which was reported in two articles ( 59 , 60 ).
A total of 152 stable outpatients and 45 acute psychotic inpatients with schizophreniform schizophrenia or brief psychotic disorder were examined. Sample sizes ranged from 15 ( 63 ) a 28 ( 58 ) in single-dose laboratory studies and 36 to 88 in longitudinal clinical trials ( 59 , 61 , 62 ). CBD studies have had heterogeneous study samples and study designs, which are reviewed below.
Regarding demographics, several studies have had samples of young adults with an average age below 30 years ( 35 , 59 , 60 , 63 , 64 ) and two studies reported the average age of patients to be in their 40s. The majority of participants (58-89%) were male. While most participants identified as white/Caucasian in two studies ( 61 , 62 ), the other four articles did not provide the race/ethnicity of their samples.
Two studies included outpatients using medications who had chronic diseases ( 58 , 61 , 62 ) and one study included patients using medications who were within 5 years of disease onset ( 63 , 64 ). Two studies involved chronic patients who were acute psychotic patients hospitalized at the time of participation ( 35 , 59 , 60 ), and these patients began the antipsychotic medication trial. One study appears to have included a mixed sample of outpatients with or without antipsychotic medication ( 58 ).
Three studies excluded participants with marijuana, alcohol, and other substance use or substance use disorders ( 58 – 61 ), but only one used urine drug screenings as a verification in this process ( 59 ). Two studies have allowed the use of cannabis during the trial ( 62 – 64 ). One of these two studies excluded patients who met the criteria for a current diagnosis of alcohol or substance dependence or a positive drug screening, but allowed current use of CUD and cannabis before and during the study ( 63 , 64 ). One study did not exclude those with a history of alcohol or substance use disorder, and the use of all substances was permitted during the study. 62 ). The case series did not provide information regarding the inclusion/exclusion of people with a history of alcohol or substance use disorder. 35 ). Nicotine use was generally not excluded, but only one study reported smoking status ( 61 ).
The dosage and duration of CBD treatment varied widely across studies. The dose of CBD ranged from 300 mg to 1,280 mg/day. Three RCTs and the case series provided daily doses for 4 to 6 weeks ( 35 , 59 – 62 ). Two administered a single dose ( 58 , 63 , 64 ).
Outcome measures included symptoms, side effects, cognition, 1 H-MRS and brain activation measured by fMRI. Clinical symptoms were most commonly assessed using the Brief Psychiatric Rating Scale [BPRS ( 65 )] and the Positive and Negative Symptom Scale [PANSS ( 66 )]. The effects of CBD on clinical symptoms have been reported by five studies ( 35 , 59 , 61 – 63 ). Side effects were evaluated in those same five studies. Motor side effects were commonly assessed using measures such as the Barnes Akathisia Scale [BAS ( 67 )], Simpson Angus Scale [SAS ( 68 )] and the Abnormal Involuntary Movements Scale [AIMS ( 69) )]. Cognition was assessed in five studies ( 58 , 60 – 63 ) with a variety of measures, and three included laboratory tests ( 59 , 60 , 62 , 63 ). A study evaluated the effects of CBD on fMRI activation during a verbal learning and memory task ( 63 and 1 H-MRS to measure glutamate levels in the left hippocampus ( 64 ). A variety of other measures were occasionally used, such as weight ( 59 , 62 ) and skin conductance ( 58 ).
Characteristics of THC studies
Only three publications report the effects of THC among patients with schizophrenia ( 55 – 57 ); two examining different data analyses from the same study ( 56 , 57 ). These studies included a total of 25 stable, medicated outpatients with chronic schizophrenia, with a mean patient age of 32.2 ( 57 ) and 44.5 ( 55 ). The proportion of men ranged from 58.3% ( 56 , 57 ) at 76.9% ( 55 ). The racial composition varied, with the proportion identified as Caucasian ranging from 46% ( 55 ) 100% ( 56 , 57 ).
One study excluded all substance use disorders except nicotine and caffeine ( 55 ), while the other ( 56 , 57 ) explicitly included the CUD. The participants in the D'Souza study ( 55 ) were required to abstain from caffeinated beverages, alcohol, and illicit substances from 2 weeks prior to the start of the trial until the conclusion of the study, verified by self-report and urine drug screening. In contrast, the studies by Fisher and Whitfield-Gabrieli required that patients meet the criteria for cannabis abuse and/or dependence and have used the substance in the previous month. The patients then abstained from all substances, with contingent reinforcements, except nicotine and caffeine for at least 7 days before the test sessions, which was verified using the Timeline Follow Back method ( 70 ), urine drug screenings and changes in quantitative THC in urine to ensure abstinence.
The dose of THC and the route of administration varied in these studies. One used a single dose of 2.5 mg and 5 mg of THC administered intravenously in different sessions ( 55 ). The patients in the studies by Fisher et al. and Whitfield-Gabrieli et al. smoked a single dose of cigarettes containing 3.6% THC or ingested 15 mg of THC orally on one occasion.
All three studies assessed the effects of THC on symptoms using the PANSS, as well as changes in the feeling of being "high" and other symptoms such as "panic" using a Visual Analogue Scale (VAS). Fischer et al. and Whitfield-Gabrieli et al. It also included formal measures of abstinence and craving for cannabis. The studies included measures of cognition, and two reports used fMRI to assess brain activation during a resting state ( 56 , 57 , 63 ). All studies collected blood samples to assess plasma THC, while one also collected cortisol and prolactin ( 55 ).
Study summaries
Effects of THC on Schizophrenia
A double-blind RCT evaluated the effects of intravenous THC 2.5 and 5 mg versus placebo in 13 stable, abstinent outpatients with schizophrenia or schizoaffective disorder without any substance use disorder who were stable on antipsychotic medication. The results were compared with 22 healthy participants who completed a similar protocol ( 27 ). Participants received the study medication in three sessions, separated by at least one week. Abstinence from caffeinated beverages, alcohol, and illicit drugs for 2 weeks was required before the start of the trial until the conclusion of the study, verified through self-report and urine tests for illicit drugs. Symptoms and cognitive tests were completed 10 and 30 minutes after infusion, respectively. THC resulted in a worsening of positive symptoms (80% of patients experienced a worsening of their PANNS subscale score by at least 3 points with the 2.5 mg dose). Verbal learning and recall also worsened, and these changes were more prominent in the patient group compared to the healthy participants. The effects on positive symptoms were not different by dose, while there was a dose effect on learning and recall. THC also worsened the negative symptoms. Self-reported perceptual changes by the clinician and movement symptoms (AIMS and akathisia scores). THC increased plasma prolactin and cortisol more than placebo. The requirement to abstain from smoking during the day of the test may have resulted in an exacerbation of symptoms associated with nicotine withdrawal.
Two reports have been published from a study evaluating the effect of oral THC 15 mg or smoked THC from a 3.6% NIDA joint on symptoms, cognition, and brain circuits using fMRI ( 56 , 57 ). Twelve stable, treated, and abstinent outpatients with schizophrenia and CUD were evaluated, in contrast to the D'Souza study, in which CUD was excluded. Alcohol dependence and other illicit substance use disorders were ruled out. Patients were abstinent from substances, with the exception of nicotine and caffeine, for at least 7 days prior to the MRI scans, as verified by self-report, urine drug screening, and quantitative testing three times a week. Tobacco smokers smoked a cigarette 90 minutes before the sweep. The patients completed two fMRI sessions with at least a 1-week interval between them. The first (baseline) session was completed without pharmacological manipulation. During the second (medication) session, patients were randomized to smoke a marijuana cigarette with 3.6% THC using a hookah-like device compatible with magnetic resonance imaging (MRI) immediately before the scan ( n = 6), or ingest a 15 mg THC capsule 3 hours before the scan ( n = 6). A group of 12 healthy controls also completed two scanning sessions.
The results of this study were published in two reports. In the first report ( 56 ), at the beginning of the study, patients showed reduced resting-state functional connectivity between the seed region of the bilateral nucleus accumbens (NAc) and prefrontal cortical regions involved in reward processing (i.e., anterior prefrontal cortex, orbitofrontal cortex, and ventral anterior cingulate cortex), as well as the dorsolateral prefrontal and premotor cortex, insula, and parahippocampal gyrus. Only one region, within the visual cortex, showed greater connectivity with the NAc in patients than in controls. Both smoked and oral THC increased connectivity between the nucleus accumbens and prefrontal regions, with greater connectivity associated with higher plasma THC levels in the combined patient sample (i.e., smoked cannabis and oral THC). THC was not associated with changes in symptoms or cognition, but scores were not included in the article. The craving for and withdrawal from cannabis also did not change with THC versus placebo in these abstinent participants, but scores were not reported either. Furthermore, no relationship was observed between connectivity and patients' ratings of high, liking, and desirability. The authors interpreted these findings as consistent with the hypothesis that the reward circuit is disrupted in schizophrenia and CUD, and that by improving this disruption, low-dose THC may have the potential to reduce cannabis use in this population.
In subsequent analyses, Whitfield-Gabrieli et al. ( 57 ) examined standard mode network (DMN) connectivity in the 12 patients described above. At the beginning of the study, compared to the healthy group, patients presented DMN hyperconnectivity that correlated with greater severity of positive PANSS symptoms, as well as reduced anticorrelation between the DMN and the executive control network (ECN). THC resulted in a reduction of this hyperconnectivity and increased the DMN-ECN anticorrelation. Furthermore, a stronger anticorrelation between DMN and ECN was associated with better performance on a verbal working memory task in the healthy group, but not in the patient group at baseline, and this association emerged in the patient group after THC administration. The authors interpreted their findings to indicate a possible dose effect, with a lower dose of THC providing benefits by improving circuit function.
Strengths and weaknesses of the THC study.
Only two controlled studies reported in three articles are available. Both studies have many strengths, including the use of placebo controls, careful measurement of prior THC exposure, and a healthy control comparison group, as shown in Table 1 . Additionally, the study by D'Souza et al. study ( 55 ) used two doses of THC, providing a dose-effect test. Only Whitfield-Gabrieli et al. ( 57 ) reported serum THC levels, confirming moderate increases that corresponded to the study's dosing strategy. Both studies had small sample sizes, which likely limited their ability to detect small effects. The two publications of the fMRI study did not clearly describe the randomization process, a potential source of bias, nor did they report symptoms or scores on cognitive measures; therefore, the evidence was indirect, and the study did not report any specific side effects (Tables 1). , 2 ) .
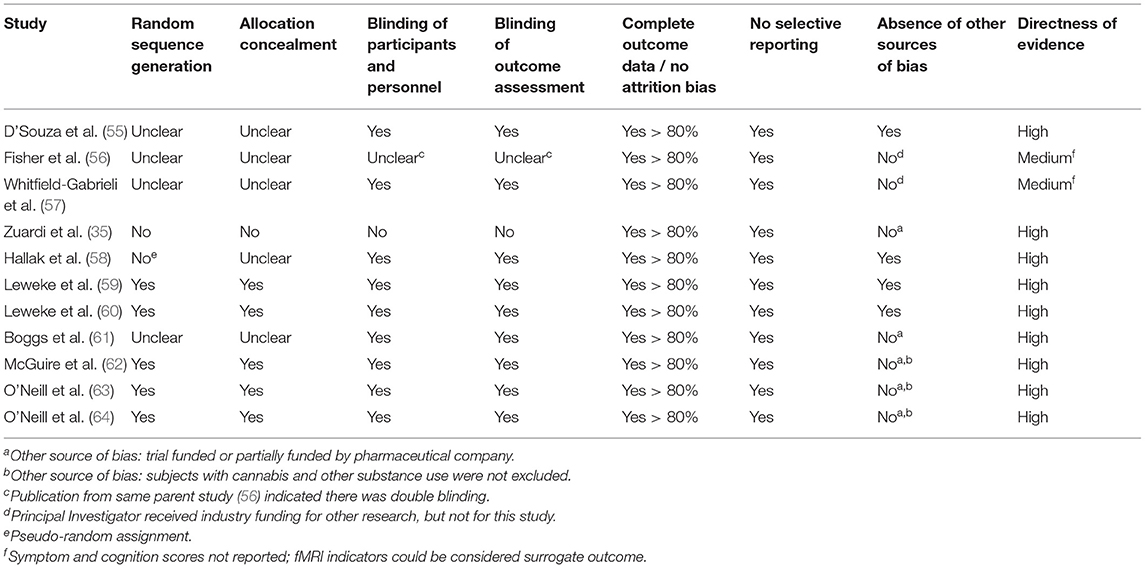
TABLE 2 . Study quality and assessment of potential for bias.
Effects of CBD on Schizophrenia
In an initial series of placebo-CBD-olanzapine crossover cases, Zuardi et al. ( 35 ) evaluated the effects of CBD on symptoms and side effects in three male patients hospitalized with treatment-resistant schizophrenia. Patients first received a placebo for 5 days, then CBD on days 6 to 35, titrated from 40 to 1,280 mg/day. On day 36, CBD was replaced with a placebo for the next 5 days and then with olanzapine for 15 days. Symptoms were systematically assessed during each treatment period. In one patient, CBD was associated with a trend toward improvement in symptoms (general, positive, and negative BPRS symptoms) at a dose of 1,280 mg/day, and symptoms worsened after discontinuation. A second patient did not benefit from CBD, although negative symptoms worsened after discontinuation. The third patient showed "minimal improvement" in symptoms. Cognition was not assessed.
Hallak et ai. ( 58 ) examined the effects of CBD 300 or 600 mg versus placebo on selective attention and electrodermal response in 28 outpatients with schizophrenia using a repeated-session, non-randomized design. Participants were assessed using the Stroop Color Word Test to evaluate selective attention, as well as the psychophysiological assessment of skin conductance, given previous research indicating that poorer selective attention is associated with low electrodermal responsiveness in patients with schizophrenia ( 71 ). The individuals were evaluated in two sessions with a 1-month interval, with the study medication administered in the second session, in which participants were classified into three groups matched by age, sex, years of schooling, and symptom profile. Each group received a single dose of placebo or 300 or 600 mg of CBD and, after 1 hour, completed the Stroop and skin conductance assessments. In contrast to the hypothetical effects, the 600 mg CBD group made more errors in the interference condition of the Stroop Color Word Test than the other two groups, reflecting poorer selective attention. Furthermore, while the placebo and 300 mg CBD groups showed improved performance in the second session compared to the first, the 600 mg CBD group did not. No psychiatric symptoms were reported. This study was limited by its very small size, and the test may have been performed before the CBD was fully absorbed.
Leweke et ai. ( 59 , 60 ) conducted a 4-week, double-blind, parallel-group, non-inferiority RCT of CBD vs. amisulpride 800 mg in four divided doses among 42 acutely psychotic inpatients with schizophrenia and no substance use disorder. After at least 3 days without antipsychotics, patients received CBD or amisulpride, titrated at 1 week and maintained at 800 mg for a further 3 weeks. The symptoms (positive, negative, and total) reported in the 2012 report improved in both groups, including a 30-point reduction in total PANSS symptom scores and approximately a nine-point reduction in positive symptoms at the 4-week endpoint. There was no difference between groups in symptom improvement, suggesting that CBD had an antipsychotic effect similar to amisulpride, although the non-inferiority test did not reach significance. 59 ). The results of a battery of cognitive tests administered before and after treatment, reported in the 2021 report, demonstrated that both groups showed improvement in visual memory and processing speed. The CBD group improved only in sustained attention and visuomotor coordination, while the amisulpride group improved in working memory. These cognitive findings, however, were not statistically significant after adjusting for multiple comparisons. 60 ). CBD was well tolerated and associated with fewer extrapyramidal symptoms, less weight gain, and less increase in prolactin than amisulpride ( 60 ). Furthermore, serum anandamide levels increased more among those treated with CBD than with amisulpride, and the extent of the increase was associated with improvement in the total PANSS score in the CBD group, but not in the amisulpride group. This finding was interpreted as suggesting a link between the antipsychotic effect of CBD and the inhibition of anandamide degradation ( 72 ). Anandamide levels and PANSS scores were not correlated with cognitive performance. The authors interpreted this finding as suggesting a different mechanism for the effect of CBD on cognition. The treatment groups were small and the study was insufficient due to enrollment challenges.
Two 6-week placebo-controlled trials evaluated the effectiveness of augmenting antipsychotics with CBD. In the first one, Boggs and colleagues ( 61 ) conducted a 6-week, double-blind, parallel-group RCT of CBD 300 mg BID vs. placebo among 36 outpatients with chronic schizophrenia and no substance use disorder in the past 3 months on a stable dose of antipsychotic medication. The average age was 48 years. Psychotic symptoms decreased over time, but the improvement was not different between treatment conditions (PANSS positive symptom scores improved by 2–3 points). In contrast to the direction of the hypothesized effect, the placebo group showed small improvements in the MCCB composite score, as well as in the Reasoning and Problem Solving domain scores. Sedation was greater (20% vs. 5%) and gastrointestinal symptoms were less frequent (33.3% vs. 55.5%) in the CBD group.
In the second 6-week augmentation study, McGuire and colleagues ( 62 ) conducted a 6-week, double-blind, parallel-group RCT with a higher dose of CBD (500 mg BID) versus placebo among a larger group of 88 patients with schizophrenia spectrum disorders, mean age 41 years, stable with at least a partial response to antipsychotic treatment. In addition to using a higher dose of CBD, this study differed from the previous study because substance use disorder was not exclusionary and the use of alcohol, marijuana, or other illicit substances was not prohibited during the study, but the DSM-5 diagnostic substance use disorder was not reported. At the start of the study, only 2.3% of the CBD group and 4.4% of the placebo group had a positive urine screening for THC, suggesting that most participants were not regular cannabis users prior to the study. Serum CBD levels were positive in all participants in the CBD group at the end of the study, suggesting adequate adherence. After the 6-week treatment phase, compared to the placebo group, the CBD group showed greater improvement in positive symptoms (reduction of 3.2 vs. 1.7 points) and was more likely to be classified as improved by the attending physician. The total change in the PANSS score was not significantly different between the groups (7.9 vs. 8.9 points). Trends were also observed in cognition (composite score and executive function domain), as well as a small but significant improvement in motor speed. Although information on substance use during the study was generally not provided, the authors reported that one patient in the CBD group was dependent on cannabis at the start of the study and did not change their pattern of use during the study. and another in the CBD group was alcohol dependent at the start of treatment, but not at the end of treatment. CBD was well tolerated, but, in contrast to Boggs' study above, CBD participants did not report drowsiness (0% vs. 6.7%) and were more likely to experience gastrointestinal side effects than the placebo group (18.6% vs. 6.7%). Since participants who used THC were not excluded and measures of THC use were not systematically assessed over time, it was not possible to rule out an interaction between the use of cannabis or other substances during the study and the effect of CBD on symptoms. 7%). Since participants who used THC were not excluded and measures of THC use were not systematically assessed over time, it was not possible to rule out an interaction between the use of cannabis or other substances during the study and the effect of CBD on symptoms. 7%). Since participants who used THC were not excluded and measures of THC use were not systematically assessed over time, it was not possible to rule out an interaction between the use of cannabis or other substances during the study and the effect of CBD on symptoms.
O'Neill et al. ( 63 , 64 ) evaluated the effect of a single dose boost with 600 mg of CBD versus placebo on symptoms, fMRI assessments of mediotemporal and prefrontal cortex activation (primarily the middle and inferior frontal gyri), as well as mediotemporal-striatal connectivity function during verbal recall, and 1. H-MRS assessment of hippocampal glutamate levels (which was corrected for cerebrospinal fluid content of the hippocampal region of interest). They studied 13 outpatients with schizophrenia (within 5 years of illness onset; mean age 28 years) in a double-blind, repeated-measures, within-subject crossover design. Patients with CUD were allowed, while alcohol and other substance dependence were excluded, as were those who were intoxicated or had a positive urine drug screening for other drugs on the day of the examination. More than half (57.1%) of the patients used marijuana. Nineteen healthy comparison (HC) participants also completed two sessions, but without medication administration for the fMRI study.
CBD was associated with a trend toward a reduction in the median total PANSS score, but not with changes in anxiety status or performance on paired verbal learning tasks. Compared to the healthy group, patients showed abnormal activation in the prefrontal region during encoding, while during recall they showed abnormal prefrontal and mediotemporal activation, as well as greater hippocampal-striatal functional connectivity. CBD partially normalized activations in these regions, as well as reduced functional hippocampal-striatal hyperconnectivity. The researchers interpreted their findings to indicate that changes in these regions are behind the antipsychotic effects of CBD.
Furthermore, in a follow-up report, O'Neill et al. ( 64 They observed a significant increase in glutamate levels in the left hippocampus in the CBD group compared to the placebo group. No group differences were observed for other metabolite levels, including glutamate-glutamine, myo-inositol, N-acetyl aspartate, and glycerophosphocholine. A multivariate model adjusted for baseline PANSS scores demonstrated a significant inverse predictive relationship between glutamate levels, but not CBD status, and total PANSS scores. The authors interpreted these findings as supporting the possibility that CBD may produce an antipsychotic effect by modulating glutamate levels in the hippocampus.
The study sample size was small, but the authors provided a power calculation indicating adequate power for the fMRI study. The design included adequate time for CBD absorption, allowing for the detection of the drug's effect. However, since half of the participants were using recreational cannabis, the authors could not determine whether the improvements associated with CBD were due to the improvement of THC-induced impairments versus impairments fundamental to schizophrenia.
Strengths and weaknesses of the CBD study.
All five studies had considerable strengths with prospective randomized assignment, a control or comparison condition, and systematic assessment of symptoms and/or cognition. The 4- and 6-week trials also carefully measured the impact on movement disorders and adverse effects. In single-dose trials, a study may not have included adequate time for absorption of oral CBD. The different characteristics of the sample (age, presence of CUD or recent cannabis use), different doses of CBD, duration of treatment, outcome measures, and timing of assessments may contribute to the heterogeneity of the results. A notable aspect of the heterogeneity in study design is the inclusion or exclusion of CUD and/or cannabis use during the study; Both studies with positive findings did not omit participants with CUD. The small sample sizes of these studies limited their ability to detect small to medium-sized effects. Boggs' study did not clearly describe the randomization process, and the pharmaceutical company's funding for some of these studies may contribute to some potential bias in the findings ( Table 2) . ).
Discussion
THC, psychotic symptoms, cognition, and adverse effects
To date, controlled laboratory studies have used heterogeneous methodology and reported different results. The D'Souza study, which was carefully designed to assess symptoms, documented an increase in positive, negative, and general symptoms of psychosis, as well as cognitive impairment, when intravenous THC was administered to patients with schizophrenia. Although there was a clear dose-response effect for learning and recall, there was no clear dose-response effect for positive symptoms. 55 ). These results are consistent with findings in healthy individuals, where 15 trials demonstrated that THC can induce psychosis in many people ( 28 ).
In contrast, the other study, which included patients with schizophrenia with concomitant CUD, reported no changes in symptoms with the administration of a modest dose of oral and smoked THC; THC significantly increased serum THC and resulted in a tendency toward tachycardia, as expected. This study demonstrated that THC reduced functional resting-state hyperconnectivity in DMN regions and improved DMN-ECN anticorrelation in brain circuits associated with schizophrenia symptomatology. 57 ), an effect opposite to what one might expect if THC worsened psychosis.
DMN hyperconnectivity has been reported in patients with schizophrenia ( 74) medicated (73) and not medicated ( 74 ) that do not have CUD. The decrease in DMN-ECN anticorrelation found was also documented in medication-naive patients ( 74 – 76 ) and chronic patients who take medication ( 73 , 77 , 78 ). Thus, the authors stated that these abnormalities may be central characteristics of schizophrenia. They interpreted their findings to indicate that THC may have a dose-dependent effect, with low doses providing benefits to brain circuits involved in psychosis and higher doses causing disturbances. The other report from this study showed a normalization of resting-state activity in circuits involved with reward ( 56 ) and proposed that a low dose of THC could also have therapeutic potential to reduce cannabis use in patients with schizophrenia and concomitant CUD.
Regarding the effect of THC on cognition in schizophrenia, intravenous THC worsened learning and recall in patients with schizophrenia without substance use disorder, with a dose-response effect where 5 mg had a greater effect than 2.5 mg ( 55 ). Although the Whitfield-Gabrielli study in abstinent patients with CUD reported that THC improved the anticorrelation between DMN and ECN, and the magnitude of the anticorrelation between DMN and ECN correlated with working memory performance, cognitive scores in relation to THC versus placebo were not reported. The effect of THC in the D'Souza study is consistent with findings that THC acutely worsens cognition in the general population ( 55 ), as well as a meta-analysis indicating better neuropsychological functioning in schizophrenia patients with a history of lifetime cannabis use, but not in those with current or recent use, compared to patients without concomitant cannabis use ( 79 ).
In addition to the dose-differential effect suggested by Whitfield-Gabrielli et al. ( 57 Other possible explanations for the different findings of symptoms and cognition in relation to THC and psychotic symptoms in these chronic schizophrenia studies include the possibility that patients with schizophrenia and concomitant CUD may be less susceptible to the psychotomimetic effects of THC than those without CUD, either due to different underlying biological risks, a notion that others have proposed ( 80 ), or due to the development of neural adaptations that result in tolerance to this effect after prolonged cannabis use. Regarding the heterogeneous biological risk for psychosis, interindividual susceptibility to THC-induced psychotic symptoms was observed in people without psychotic disorders ( 27 , 81 ). Assuming that this heterogeneity also exists in people with schizophrenia, it is possible that those with less susceptibility to symptom exacerbation are more likely to develop a CUD, as they would not suffer immediate negative consequences from THC use. The problematic course of illness associated with CUD in schizophrenia may be due to the more general detrimental impact of substance use disorders in schizophrenia, including non-adherence to medication ( 82 – 84 ). Alternatively, people with schizophrenia and CUD may have developed a tolerance to the psychotoxic effects of THC, as has been demonstrated in people without psychotic disorders ( 81 , 85 ).
CBD, psychotic symptoms, cognition, and side effects
Controlled prospective research on the impact of CBD to date is mixed. The small study comparing 800 mg of CBD with amisulpride among 42 symptomatic, unmedicated hospitalized patients (mean age 30 years) with negative THC tests and substance use disorder demonstrated a 30-point reduction in total PANSS scores at 4 weeks and approximately a 9-point reduction in positive psychosis symptoms in both groups. 59 ). Although this study did not have a placebo control group, the results strongly suggest that CBD has an antipsychotic effect. A recent article also reported cognitive assessments from the same study, indicating similar levels of improvement with CBD and amisulpride, but without statistical significance after correction for multiple comparisons. 60 ). The four small placebo-controlled studies of CBD augmentation in schizophrenia provide mixed and limited support for the ability of CBD added to an antipsychotic to further reduce symptoms of psychosis and improve cognitive impairments. In contrast to research on THC, this research demonstrated that CBD did not worsen psychosis or cognition compared to placebo.
These inconsistent results regarding the potential beneficial effects of CBD may be due to different CBD doses, different patient ages, and the presence of recent/current recreational THC and other substance exposures in these studies. Between the two 6-week augmentation trials, the study that demonstrated a positive effect on symptoms and cognition ( 62 ) used a higher dose of CBD (1,000 mg vs. 600 mg) and enrolled individuals with a lower average age (41 vs. 48 years). Therefore, it is possible that a higher dose may be needed or that younger patients may respond better to CBD. The findings on the effect of CBD using fMRI in the studies reviewed here ( 63 ), which also recruited young individuals, are similar to recent fMRI studies in young, antipsychotic-naive adults with a high clinical risk of psychosis. These trials found partial normalization of the circuits involved in verbal learning and memory ( 86 ) and motivational relevance ( 87 ) after a single dose of CBD. The new discoveries of 1 H-MRS suggests a possible mechanism for the impact of CBD on schizophrenia symptoms ( 64 ). Together, these findings suggest that the effects of CBD on brain function in schizophrenia cannot be easily explained by disease-related factors such as medication history and chronicity.
One point of significant interest is that studies have found a positive effect for increasing CBD ( 62 – 64 They did not omit participants with CUD or current cannabis use and did not carefully measure cannabis use during the study period. Previous research has shown that CBD in robust doses can attenuate THC-induced psychotic symptoms in healthy individuals ( 29 , 30 ). Thus, it is possible that CBD was influencing THC-induced deficiencies rather than deficiencies due to schizophrenia in these two studies with positive results. It is also possible that people with schizophrenia who use cannabis or have a CUD may respond differently to CBD than those who do not have a CUD, but no studies have carefully examined the effect of CBD in patients with schizophrenia and CUD. Furthermore, we found no published laboratory studies testing the combination of CBD with THC in schizophrenia, nor among those with co-occurring CUD. Patients with co-occurring disorders are of particular interest, given preliminary findings that low doses of THC normalized resting-state functional connectivity in areas related to reward processing and executive control without increasing symptoms or worsening cognition ( 56 , 57 ).
This review is limited by the small number of controlled studies available on the subject, but the consideration of CBD and THC studies, along with a careful review of the methodology and study results, provides an important current assessment of the evidence on the effect of cannabis on schizophrenia. It is important to emphasize that previous reviews did not take into account whether patients were using alcohol or substances of abuse (including marijuana) at the time of participation and/or had a prior history of alcohol or substance use disorder. A history of alcohol/substance use may be especially important to consider, as it can affect the results of THC or CBD tests in schizophrenia. This possibility is raised by research indicating differential effects of acute cannabinoid administration on cognition ( 88 , 89 ) and classifications of intoxication ( 90 , 91 ) in frequent and infrequent cannabis users without schizophrenia, as well as a higher initial peak plasma THC level in frequent users ( 90 , 92 ).
Overall, there is insufficient evidence regarding the ability of THC or CBD to affect symptoms and cognition in patients with schizophrenia, so neither cannabinoid should be recommended to treat this group until further research provides a clearer picture of their impact on this disease and among people who have both schizophrenia and CUD. In the era of legalization, public health authorities could consider whether there is sufficient evidence related to THC (from a high-quality laboratory study consistent with epidemiological research and effects in people without psychotic disorders) to provide public warnings that THC may worsen symptoms among some people with schizophrenia. Studying the effect of THC and CBD on schizophrenia is a challenge.
Data Availability Statement
The original contributions presented in the study are included in the supplementary article/material; further questions may be directed to the corresponding author(s).
Author's contributions
CS and MB determined the study design and contributed to the development of the original protocol. SA and CS contributed to the original screening of articles, data extraction, and drafting of the first manuscript. RR contributed to the study design. MB and RR conducted the analysis, interpretation of the literature review, and critical review of the manuscript. MB, RR, and SA contributed to the editing of the final version. All authors approved the final version.
Financing
This work was funded in part by a grant from the National Institute on Drug Abuse to MB (1R01DA034699-01).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be interpreted as a potential conflict of interest.
Editor's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, editors, and reviewers. Any product that may be reviewed in this article, or any claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to thank Karen Goodman, MSLIS, MA, medical librarian at the Dorothy M. Breene Memorial Library at New Hampshire Hospital, for her assistance in the bibliographic research and obtaining the articles necessary for this paper.
References
1. Black DW, Andreasen NC. Introductory treatise on psychiatry . Arlington, VA: American Psychiatric Pub (2011).
2. Mueser KT, McGurk SR. Schizophrenia. Lancet. (2004) 363:2063–72. doi: 10.1016/S0140-6736(04)16458-1
3. Gold JM, Waltz JA, Prentice KJ, Morris SE, Heerey EA. Reward processing in schizophrenia: a deficit in value representation. Schizophrenic Taurus. (2008) 34:835–47. doi: 10.1093/schbul/sbn068
4. Achim AM, Maziade M, Raymond É, Olivier D, Mérette C, Roy -A, et al. What is the prevalence of anxiety disorders in schizophrenia? A meta-analysis and critical review of a significant association. Schizophrenic Taurus. (2011) 37:811–21. doi: 10.1093/schbul/sbp148
5. Kiran C, Chaudhury S. Prevalence of comorbid anxiety disorders in schizophrenia. Ind Psychiatry J . (2016) 25:35. doi: 10.4103/0972-6748.196045
6. Green B, Young R, Kavanagh D. Prevalence of marijuana use and abuse among people with psychosis. Br J Psychiatry. (2005) 187:306–13. doi: 10.1192/bjp.187.4.306
7. Mueser KT, Yarnold PR, Rosenberg SD, Swett Jr C, Miles KM, Hill D. Substance use disorder in severely mentally ill hospitalized psychiatric patients: prevalence, correlates, and subgroups. Schizophrenic Taurus. (2000) 26:179–92. doi: 10.1093/oxfordjournals.schbul.a033438
8. Ringen P, Lagerberg T, Birkenaes A, Engn J, Faerden A, Jonsdottir H, et al. Differences in prevalence and patterns of substance use in schizophrenia and bipolar disorder. Medical Psychology (2008) 38:1241. doi: 10.1017/S003329170700236X
9. Sevy S, Robinson DG, Holloway S, Alvir JM, Woerner MG, Bilder R, et al. Correlates of substance misuse in patients with first-episode schizophrenia and schizoaffective disorder. Acta Psychiatr Scand. (2001) 104:367–74. doi: 10.1111/j.1600-0447.2001.00452.x
10. Green AI, Noordsy DL, Brunette MF, O'Keefe C. Substance abuse and schizophrenia: pharmacotherapeutic intervention. J Subst Abuse Treat. (2008) 34:61–71. doi: 10.1016/j.jsat.2007.01.008
11. Henquet C, Murray R, Linszen D, van Os. J. The environment and schizophrenia: the role of cannabis use. Schizophrenic Taurus. (2005) 31:608–12. doi: 10.1093/schbul/sbi027
12. Koskinen J, Löhönen J, Koponen H, Isohanni M, Miettunen J. Rate of cannabis use disorders in clinical samples of patients with schizophrenia: a meta-analysis. Schizophrenic Taurus. (2010) 36:1115–30. doi: 10.1093/schbul/sbp031
13. Regier DA, Farmer ME, Rae DS, Locke BZ, Keith SJ, Judd LL, et al. Comorbidity of mental disorders with alcohol and other drug abuse: results from the Epidemiologic Catchment Area (ECA) study. JAMA. (1990) 264:2511-8. doi: 10.1001/jama.1990.03450190043026
14. Hasin DS, Kerridge BT, Saha TD, Huang B, Pickering R, Smith SM, et al. Prevalence and correlates of DSM-5 cannabis use disorder, 2012-2013: results from the National Epidemiological Survey on Alcohol and Related Conditions – III. Am J Psychiatry . (2016) 173:588–99. doi: 10.1176/appi.ajp.2015.15070907
15. Arseneault L, Cannon M, Poulton R, Murray R, Caspi A, Moffitt TE. Cannabis use in adolescence and risk of psychosis in adults: a prospective longitudinal study. BM J. (2002) 325:1212–13. doi: 10.1136/bmj.325.7374.1212
16. Griffith-Lendering M, Wigman J, Prince van Leeuwen A, Huijbregts S, Huizink AC, Ormel J, et al. Cannabis use and vulnerability to psychosis in early adolescence – a TRAILS study. Addiction. (2013) 108:733–40. doi: 10.1111/add.12050
17. Marconi A, Di Forti M, Lewis CM, Murray RM, Vassos E. Meta-analysis of the association between cannabis use level and risk of psychosis. Schizophrenic Taurus. (2016) 42:1262–9. doi: 10.1093/schbul/sbw003
18. Miettunen J, Törmänen S, Murray GK, Jones PB, Mäki P, Ebeling H, et al. Association between cannabis use and prodromal symptoms of psychosis in adolescence. Br J Psychiatry. (2008) 192:470–1. doi: 10.1192/bjp.bp.107.045740
19. Stefanis N, Delespaul P, Henquet C, Bakoula C, Stefanis C, Van Os J. Early exposure to cannabis in adolescence and positive and negative dimensions of psychosis. Addiction. (2004) 99:1333–41. doi: 10.1111/j.1360-0443.2004.00806.x
20. Ben-Zeev D, Ellington K, Swendsen J, Granholm E. Examining a cognitive model of persecutory ideation in the daily lives of people with schizophrenia: a computerized experience sampling study. Schizophrenic Taurus. (2011) 37:1248–56. doi: 10.1093/schbul/sbq041
21. Buckley PF, Miller BJ, Lehrer DS, Castle DJ. Psychiatric comorbidities and schizophrenia. Schizophrenic Taurus. (2009) 35:383–402. doi: 10.1093/schbul/sbn135
22. Henquet C, van Os J, Kuepper R, Delespaul P, Smits M, Campo JA, et al. Psychosis reactivity to cannabis use in daily life: an experience sampling study. Br J Psychiatry. (2010) 196:447–53. doi: 10.1192/bjp.bp.109.072249
23. Zammit S, Moore TH, Lingford-Hughes A, Barnes TR, Jones PB, Burke M, et al. Effects of cannabis use on outcomes in psychotic disorders: a systematic review. Br J Psychiatry. (2008) 193:357–63. doi: 10.1192/bjp.bp.107.046375
24. Hasin DS. Epidemiology of cannabis use in the US and associated problems. Neuropsychopharmacology. (2018) 43:195–212. doi: 10.1038/npp.2017.198
25. Babalonis S, Haney M, Malcolm RJ, Lofwall MR, Votaw VR, Sparenborg S, et al. Oral cannabidiol does not produce a risk signal for abuse in frequent marijuana smokers. Drugs, alcohol, it depends. (2017) 172:9–13. doi: 10.1016/j.drogalcdep.2016.11.030
26. Haney M, Malcolm RJ, Babalonis S, Nuzzo PA, Cooper ZD, Bedi G, et al. Oral cannabidiol does not alter the subjective, enhancing, or cardiovascular effects of smoked cannabis. Neuropsychopharmacology. (2016) 41:1974–82. doi: 10.1038/npp.2015.367
27. D'Souza DC, Perry E, MacDougall L, Ammerman Y, Cooper T, Braley G, et al. The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology. (2004) 29:1558–72. doi: 10.1038/sj.npp.1300496
28. Sherif M, Radhakrishnan R, D'Souza DC, Ranganathan M. Human laboratory studies on cannabinoids and psychosis. Biological Psychiatry (2016) 79:526–38. doi: 10.1016/j.biopsych.2016.01.011
29. Bhattacharyya S, Morrison PD, Fusar-Poli P, Martin-Santos R, Borgwardt S, Winton-Brown T, et al. Opposing effects of Δ-9-tetrahydrocannabinol and cannabidiol on human brain function and psychopathology. Neuropsychopharmacology. (2010) 35:764–74. doi: 10.1038/npp.2009.184
30. Englund A, Morrison PD, Nottage J, Hague D, Kane F, Bonaccorso S, et al. Cannabidiol inhibits THC-induced paranoid symptoms and hippocampus-dependent memory impairment. J Psychopharmacol. (2013) 27:19–27. doi: 10.1177/0269881112460109
31. Leweke FM, Schneider U, Radwan M, Schmidt E, Emrich HM. Different effects of nabilone and cannabidiol on binocular depth inversion in humans. Pharmacol Biochem Behav. (2000) 66:175–81. doi: 10.1016/S0091-3057(00)00201-X
32. Schubart CD, Sommer IE, van Gastel WA, Goetgebuer RL, Kahn RS, Boks MP. Cannabis with a high cannabidiol content is associated with fewer psychotic experiences. Schizophrenic Res. (2011) 130:216–21. doi: 10.1016/j.schres.2011.04.017
33. ElSohly MA, Mehmedic Z, Foster S, Gon C, Chandra S, Church JC. Changes in cannabis potency over the last 2 decades (1995–2014): analysis of current data in the United States. Biological Psychiatry (2016) 79:613–9. doi: 10.1016/j.biopsych.2016.01.004
34. Bidwell LC, Mueller R, YorkWilliams SL, Hagerty S, Bryan AD, Hutchison KE. A novel observational method for assessing acute responses to cannabis: preliminary validation using legal strains from the market. Cannabis Cannabinoid Res. (2018) 3:35–44. doi: 10.1089/can.2017.0038
35. Zuardi AW, Crippa J, Hallak J, Moreira F, Guimarães F. Cannabidiol, a constituent of Cannabis sativa, as an antipsychotic drug. Brazilian Journal of Medical Biol Res. (2006) 39:421–9. doi: 10.1590/S0100-879X2006000400001
36. Zuardi AW, Morais S, Guimarães F, Mechoulam R. Antipsychotic effect of cannabidiol. Psychiatry J Clin. (1995) 56:485-6.
38. Keyhani S, Steigerwald S, Ishida J, Vali M, Cerdá M, Hasin D, et al. Risks and benefits of marijuana use: a national survey of American adults. Ann Intern Med. (2018) 169:282–9 doi: 10.7326/M18-0810
39. Reinarman C, Nunberg H, Lanthier F, Heddleston T. Who are medical marijuana patients? Characteristics of the population of nine evaluation clinics in California. J Psychoact Drugs. (2011) 43:128–35. doi: 10.1080/02791072.2011.587700
40. Adlaf EM, Begin P, Sawka E. Canadian Addiction Survey (CAS): A National Survey of Alcohol and Other Drug Use by Canadians: Prevalence of Use and Related Harms: Detailed Report . Ottawa, ON: Canadian Centre on Substance Abuse (2005).
41. Walsh Z, Callaway R, Belle-Isle L, Capler R, Kay R, Lucas P, et al. Cannabis for therapeutic purposes: patient characteristics, access, and reasons for use. International Drug Policy J. (2013) 24:511–6. doi: 10.1016/j.drugpo.2013.08.010
42. Wigman JT, van Nierop M, Vollebergh WA, Lieb R, Beesdo-Baum K, Wittchen U, et al. Evidence suggests that psychotic symptoms are prevalent in anxiety and depression disorders, impacting the onset, risk, and severity of the illness—implications for diagnosis and ultra-high-risk research. Schizophrenic Taurus. (2012) 38:247–57. doi: 10.1093/schbul/sbr196
43. Bartoli F, Riboldi I, Bachi B, Calabrese A, Moretti F, Crocamo C, et al. Efficacy of cannabidiol for psychotic symptoms induced by δ-9-tetrahydrocannabinol, schizophrenia, and cannabis use disorders: a narrative review. J Clin Med. (2021) 10:1303. doi: 10.3390/jcm10061303
44. Batalla A, Janssen H, Gangadin SS, Bossong MG. The potential of cannabidiol as a treatment for psychosis and addiction: who benefits most? A systematic review. J Clin Med. (2019) 8:1058. doi: 10.3390/jcm8071058
45. Bonaccorso S, Ricciardi A, Zangani C, Chiappini S, Schifano F. Use of cannabidiol (CBD) in psychiatric disorders: a systematic review. Neurotoxicology. (2019) 74:282–98. doi: 10.1016/j.neuro.2019.08.002
46. Davies C, Bhattacharyya S. Cannabidiol as a potential treatment for psychosis. Ther Adv Psychopharmacol. (2019) 9:2045125319881916. doi: 10.1177/2045125319881916
47. Ghabrash MF, Coronado-Montoya S, Aoun J, Gagné A.-A., Mansour F, et al. Cannabidiol for the treatment of psychosis among patients with schizophrenia and other primary psychotic disorders: a systematic review with risk of evaluation bias. Psychiatry Resolution. (2020) 286:112890. doi: 10.1016/j.psychres.2020.112890
48. Osborne AL, Solowij N, Weston-Green K. A systematic review of the effect of cannabidiol on cognitive function: relevance to schizophrenia. Neurosci Biobehav Rev. (2017) 72:310–24. doi: 10.1016/j.neubiorev.2016.11.012
49. Saeed SA, Clary KE. Cannabidiol for psychosis: a review of 4 studies. Curr Psychiatr. (2020) 19:24–31. doi: 10.12788/cp.0002
50. Schoevers J, Leweke JE, Leweke FM. Cannabidiol as a treatment option for schizophrenia: recent evidence and current studies. Curr Opin Psychiatry. (2020) 33:185–91. doi: 10.1097/YCO.0000000000000596
51. Meader N, King K, Llewellyn A, Norman G, Brown J, Rodgers M, et al. A checklist designed to aid in the consistency and reproducibility of GRADE assessments: development and pilot validation. Syst Rev. (2014) 3:1–9. doi: 10.1186/2046-4053-3-82
52. Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello P, et al. GRADE Guidelines: 4. Assessment of the quality of evidence — study limitations (risk of bias). J Clin Epidemiol. (2011) 64:407–15. doi: 10.1016/j.jclinepi.2010.07.017
53. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on classifying the quality of evidence and the strength of recommendations. Bmj. (2008) 336:924–6. doi: 10.1136/bmj.39489.470347.AD
54. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration tool for assessing the risk of bias in randomized trials. BMJ . (2011) 343:d5928. doi: 10.1136/bmj.d5928
55. D'Souza DC, Abi-Saab WM, Madonick S, Forselius-Bielen K, Doersch A, Braley G, et al. Effects of delta-9-tetrahydrocannabinol in schizophrenia: implications for cognition, psychosis, and addiction. Biological Psychiatry (2005) 57:594–608. doi: 10.1016/j.biopsych.2004.12.006
56. Fischer AS, Whitfield-Gabrieli S, Roth RM, Brunette MF, Green AI. Impaired functional connectivity of the brain's reward circuit in patients with schizophrenia and cannabis use disorder: effects of cannabis and THC. Schizophrenic Res. (2014) 158:176–82. doi: 10.1016/j.schres.2014.04.033
57. Whitfield-Gabrieli S, Fischer AS, Henricks AM, Khokhar JY, Roth RM, Brunette MF, et al. Understanding the effects of marijuana on functional default mode network connectivity in patients with schizophrenia and concomitant cannabis use disorder: a pilot investigation. Schizophrenic Res. (2018) 194:70–7. doi: 10.1016/j.schres.2017.07.029
58. Hallak JE, Machado-de-Sousa JP, Crippa JAS, Sanches RF, Trzesniak C, Chaves C, et al. Performance of schizophrenic patients on the Stroop Color Word Test and electrodermal responsiveness after acute administration of cannabidiol (CBD). Psychiatry Braz J. (2010) 32:56–61. doi: 10.1590/S1516-44462010000100011
59. Leweke F, Piomelli D, Pahlisch F, Muhl D, Gerth C, Hoyer C, et al. Cannabidiol increases anandamide signaling and alleviates the psychotic symptoms of schizophrenia. Transl Psychiatry. (2012) 2:e94. doi: 10.1038/tp.2012.15
60. Leweke FM, Rohleder C, Gerth CW, Hellmich M, Pukrop R, Koethe D. Cannabidiol and amisulpride improve cognition in acute schizophrenia in an exploratory, double-blind, active-controlled randomized clinical trial. Front Farmacol . (2021) 12:614811. doi: 10.3389/fphar.2021.614811
61. Boggs DL, Nguyen JD, Morgenson D, Taffe MA, Ranganathan M. Clinical and preclinical evidence for functional interactions of cannabidiol and Δ9-tetrahydrocannabinol. Neuropsychopharmacology. (2018) 43:142–54. doi: 10.1038/npp.2017.209
62. McGuire P, Robson P, Cubala WJ, Vasile D, Morrison PD, Barron R, et al. Cannabidiol (CBD) as adjunctive therapy in schizophrenia: a multicenter randomized controlled trial. Am J Psychiatry. (2018) 175:225–31. doi: 10.1176/appi.ajp.2017.17030325
63. O'Neill A, Wilson R, Blest-Hopley G, Annibale L, Colizzi M, Brammer M, et al. The normalization of mediotemporal and prefrontal activity, and mediotemporal-striatal connectivity, may underlie the antipsychotic effects of cannabidiol in psychosis. Psychol Med . (2020) 51:596–606. doi: 10.1017/S0033291719003519
64. O'Neill A, Annibale L, Blest-Hopley G, Wilson R, Giampietro V, Bhattacharyya S. Cannabidiol modulation of hippocampal glutamate in early psychosis. J Psychopharmacol . 32:56–61. (2021). doi: 10.1177/02698811211001107
65. General JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep. (1962) 10:799–812. doi: 10.2466/pr0.1962.10.3.799
66. Kay SR, Fiszbein A, Opler LA. The Positive and Negative Syndrome Scale (PANSS) for schizophrenia. Schizophrenic Taurus. (1987) 13:261. doi: 10.1093/schbul/13.2.261
67. Barnes TR. A rating scale for drug-induced akathisia. Br J Psychiatry. (1989) 154:672–76. doi: 10.1192/bjp.154.5.672
68. Hawley C, Fineberg N, Roberts A, Baldwin D, Sahadevan A, Sharman V. The use of the Simpson Angus Scale for the assessment of movement disorders: a training guide. International Journal of Psychiatry Clinical Practice (2003) 7:349–2257. doi: 10.1080/13651500310002986
69. Munetz MR, Benjamin S. How to examine patients using the Abnormal Involuntary Movement Scale. Psychiatric Service. (1988) 39:1172–7. doi: 10.1176/ps.39.11.1172
70. Sobell LC, Sobell MB. Timeline tracking. In: Litten R and Allen J, editors. Measuring Alcohol Consumption . Totowa, NJ: Humana Press (1992). page. 41–72.
71. Lopes-Machado EZ, de Souza Crippa JA, Hallak JEC, Guimarães FS, Zuardi AW. Patients with schizophrenia who do not respond to electrodermal stimulation make more errors on the Stroop Color Word Test, indicating a deficit in selective attention. Schizophrenic Taurus. (2002) 28:459–66. doi: 10.1093/oxfordjournals.schbul.a006953
72. Bisogno T, Hanuš L, De Petrocellis L, Tchilibon S, Ponde DE, Brandi I, et al. Molecular targets for cannabidiol and its synthetic analogues: effect on vanilloid VR1 receptors and on cellular uptake and enzymatic hydrolysis of anandamide. Br J Pharmacol. (2001) 134:845–52. doi: 10.1038/sj.bjp.0704327
73. Zhou Y, Liang M, Tian L, Wang K, Hao Y, Liu H, et al. Functional disintegration in paranoid schizophrenia using resting-state fMRI. Schizophrenic Res. (2007) 97:194–205. doi: 10.1016/j.schres.2007.05.029
74. Whitfield-Gabrieli S, Thermenos HW, Milanovic S, Tsuang MT, Faraone SV, McCarley RW, et al. Hyperactivity and hyperconnectivity of the standard network in schizophrenia and in first-degree relatives of people with schizophrenia. Proc Nat Acad Sci. (2009) 106:1279–84. doi: 10.1073/pnas.0809141106
75. Hamilton LS, Altshuler LL, Townsend J, Bookheimer SY, Phillips OR, Fischer J. Changes in functional activation in euthymic bipolar disorder and schizophrenia during a working memory task. Hum Brain Mapp. (2009) 30:3958–69. doi: 10.1002/hbm.20820
76. Ortiz-Gil J, Pomarol-Clotet E, Salvador R, Canales-Rodríguez EJ, Sarro S, Gomar JJ, et al. Neural correlates of cognitive impairment in schizophrenia. Br J Psychiatry. (2011) 199:202–10. doi: 10.1192/bjp.bp.110.083600
77. Repovs G, Csernansky JG, Barch DM. Brain network connectivity in individuals with schizophrenia and their siblings. Biological Psychiatry (2011) 69:967–73. doi: 10.1016/j.biopsych.2010.11.009
78. Woodward ND, Rogers B, Heckers S. Resting-state functional networks are affected differently in schizophrenia. Schizophrenic Res. (2011) 130:86–93. doi: 10.1016/j.schres.2011.03.010
79. Yücel M, Bora E, Lubman DI, Solowij N, Brewer WJ, Cotton SM, et al. The impact of cannabis use on cognitive functioning in patients with schizophrenia: a meta-analysis of existing findings and new data in a first-episode sample. Schizophrenic Taurus. (2012) 38:316–30. doi: 10.1093/schbul/sbq079
80. Sami MB, Bhattacharyya S. Are cannabis users and non-users different groups? To understand the neurobiology of cannabis use in psychotic disorders. J Psychopharmacol. (2018) 32:825–49. doi: 10.1177/0269881118760662
81. Morrison P, Zois V, McKeown D, Lee T, Holt D, Powell J, et al. The acute effects of synthetic intravenous [Delta] 9-tetrahydrocannabinol on psychosis, mood, and cognitive function. Medical Psychology (2009) 39:1607. doi: 10.1017/S0033291709005522
82. Abdel-Baki A, Ouellet-Plamondon C, Salvat É, Grar K, Potvin S. Symptomatic and functional outcomes of persistent substance use disorder 2 years after admission to a first-episode psychotic program. Psychiatry Resolution. (2017) 247:113–19. doi: 10.1016/j.psychres.2016.11.007
83. Higashi K, Medic G, Littlewood KJ, Diez T, Granström O, De Hert M. Medication adherence in schizophrenia: factors influencing adherence and consequences of non-adherence, a systematic review of the literature. Ther Adv Psychopharmacol. (2013) 3:200–18. doi: 10.1177/2045125312474019
84. Wilk J, Marcus SC, West J, Countis L, Hall R, Regier DA, et al. Substance abuse and the management of medication non-adherence in schizophrenia. J Nerv Ment Dis. (2006) 194:454–7. doi: 10.1097/01.nmd.0000221289.54911.63
85. D'souza DC, Ranganathan M, Braley G, Gueorguieva R, Zimolo Z, Cooper T, et al. Attenuated psychotomimetic and amnesic effects of Δ-9-tetrahydrocannabinol in frequent cannabis users. Neuropsychopharmacology. (2008) 33:2505–16. doi: 10.1038/sj.npp.1301643
86. Bhattacharyya S, Wilson R, Appiah-Kusi E, O'Neill A, Brammer M, Perez J, et al. Effect of cannabidiol on medial temporal, midbrain, and striatal dysfunction in people with high clinical risk of psychosis: a randomized clinical trial. JAMA Psychiatry. (2018) 75:1107–17. doi: 10.1001/jamapsychiatry.2018.2309
87. Wilson R, Bossong MG, Appiah-Kusi E, Petros N, Brammer M, Perez J, et al. Cannabidiol attenuates insular dysfunction during the processing of motivational salience in individuals at high clinical risk of psychosis. Transl Psychiatry. (2019) 9:1–10. doi: 10.1038/s41398-019-0534-2
88. Ramaekers J, Van Wel J, Spronk D, Toennes S, Kuypers K, Theunissen E, et al. Cannabis and tolerance: acute drug impairment as a function of cannabis use history. Scientific Representative (2016) 6:1–9. doi: 10.1038/srep31939
89. Sewell RA, Schnakenberg A, Elander J, Radhakrishnan R, Williams A, Skosnik PD, et al. Acute effects of THC on time perception in frequent and infrequent cannabis users. Psychopharmacology. (2013) 226:401–13. doi: 10.1007/s00213-012-2915-6
90. Fabritius M, Chtioui H, Battistella G, Annoni J.-M., Dao K, et al. Comparison of cannabinoid concentrations in oral fluid and whole blood between occasional and regular cannabis smokers before and after smoking a cannabis joint. Anal Bioanal Chem. (2013) 405:9791–803. doi: 10.1007/s00216-013-7412-1
91. Solowij N, Broyd S, Greenwood L.-,m., van Hell H, Martelozzo D, et al. A randomized controlled trial of vaporized Δ9-tetrahydrocannabinol and cannabidiol alone and in combination in frequent and infrequent cannabis users: acute intoxication effects. Eur Arch Psychiatry Clin Neurosci. (2019) 269:17–35. doi: 10.1007/s00406-019-00978-2
Keywords: Cannabis, marijuana, schizophrenia, psychosis, CBD, THC, legalization, fMRI
Quote: Ahmed S, Roth RM, Stanciu CN, and Brunette MF (2021) The impact of THC and CBD on schizophrenia: a systematic review. Front. Psychiatry 12:694394. doi: 10.3389/fpsyt.2021.694394
Received: April 13, 2021; Accepted: June 25, 2021;
Publication: July 23, 2021.
Reviewed by:
Michael Patrick Schaub , University of Zurich, SwitzerlandLiangsuo Ma , Virginia Commonwealth University, United States
Copyright © 2021 Ahmed, Roth, Stanciu and Morena. This is an open access article distributed under the terms of Creative Commons Attribution License (CC BY) . Use, distribution, or reproduction in other forums is permitted, provided that the original author(s) and copyright holder(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution, or reproduction is permitted that is not in accordance with these terms.
*Correspondence: Mary F. Brunette, mary.f.brunette@hitchcock.org
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations or those of the publisher, editors, and reviewers. Any product that may be reviewed in this article or any claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.